-
-
-
Rebates: Who Reaps the Benefits?
Much of the conversation centered on the topic of rebates – confidential discounts off the list price negotiated by either insurers or pharmacy benefit managers (PBMs) with drug manufacturers in exchange for placing those drugs on the insurer’s formulary of covered medications. Panelists debated whether these discounts – which are not directly passed through to plan participants – should be eliminated as part of a strategy for reducing out-of-pocket costs.
The panel also discussed recent calls to allow Medicare to directly negotiate drug prices.
Price Benchmarks: Looking to the World
One frequently discussed way of controlling drug prices is the use of an international price index (IPI) benchmarking system. The goal of such a model would be to reduce the price paid by Medicare for a drug by setting its target price closer to what other nations pay.
Some reservations about the efficacy and the effects of the system were raised by panelists, such as that it would be detrimental to competition and would significantly reduce investment in future therapies. And, as a recent Analysis Group article points out, even in European drug markets, where benchmark comparisons are mandatory in certain situations, determining the appropriate target prices is a highly complex undertaking.1
New Pricing Models: Netflix, Anyone?
The panel addressed whether innovative pricing methods might help ensure access to higher-priced therapies. Such models have already been proposed and debated for gene therapies – including, for example, long-term financing plans for expensive, “one and done” treatments, and agreements that link payments to therapeutic outcomes.2
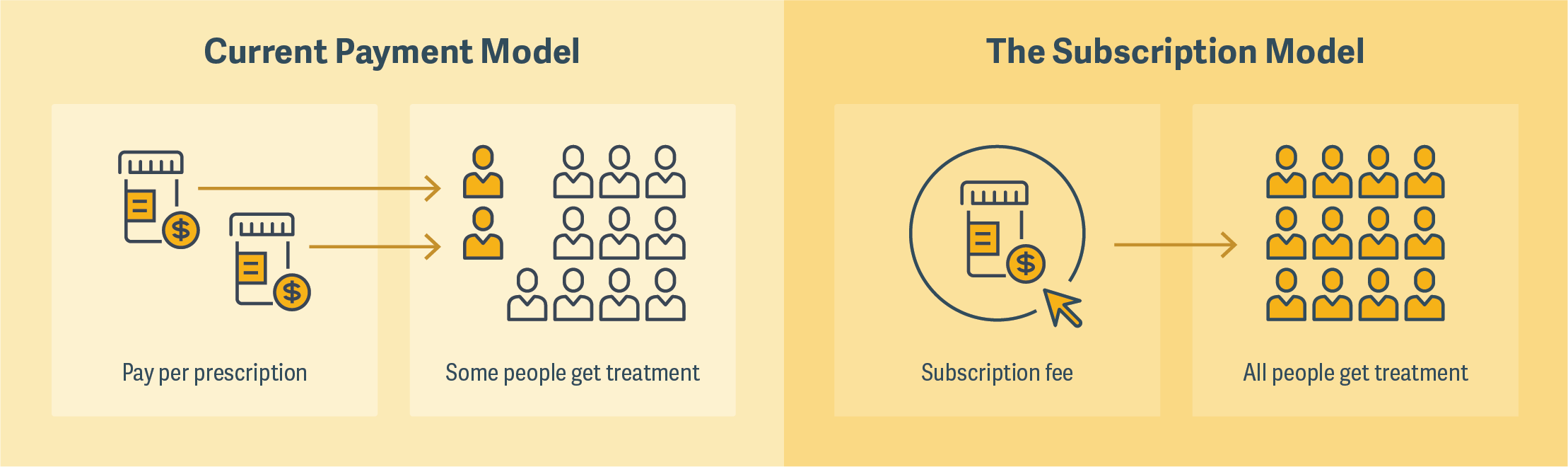
One that was much discussed by panelists was the so-called “Netflix model,” a subscription model that Louisiana has recently employed to cover hepatitis C treatments for its Medicaid and prison populations. The state agreed to pay a drug manufacturer a fixed amount and, in return, receive unlimited doses of the medication. (See figure.) The program was described by some panelists as a “win-win” because it would greatly expand the number of people who would have access to a particular treatment and give drug manufacturers certainty about revenue.
There was some discussion, however, about the conditions under which such a model could be successful, and whether it could be broadly applicable. There were also reservations expressed about the market signals that would be sent by lowering an already cost-effective price for a drug, which might in turn contribute to underinvestment by venture capital in the pharmaceutical market. ■
Click on the graphic below to view an animated version
-
